|
Key Takeaways:
Cataract → blurry/foggy vision, glare/halos at night, faded colours, frequent glasses changes.
Cataract usually worsens slowly over the years and is reversible with surgery.
Cataract: vision chart, slit-lamp and dilated lens exam.
Cataract → remove cloudy lens and place a clear IOL (day-care surgery).
|
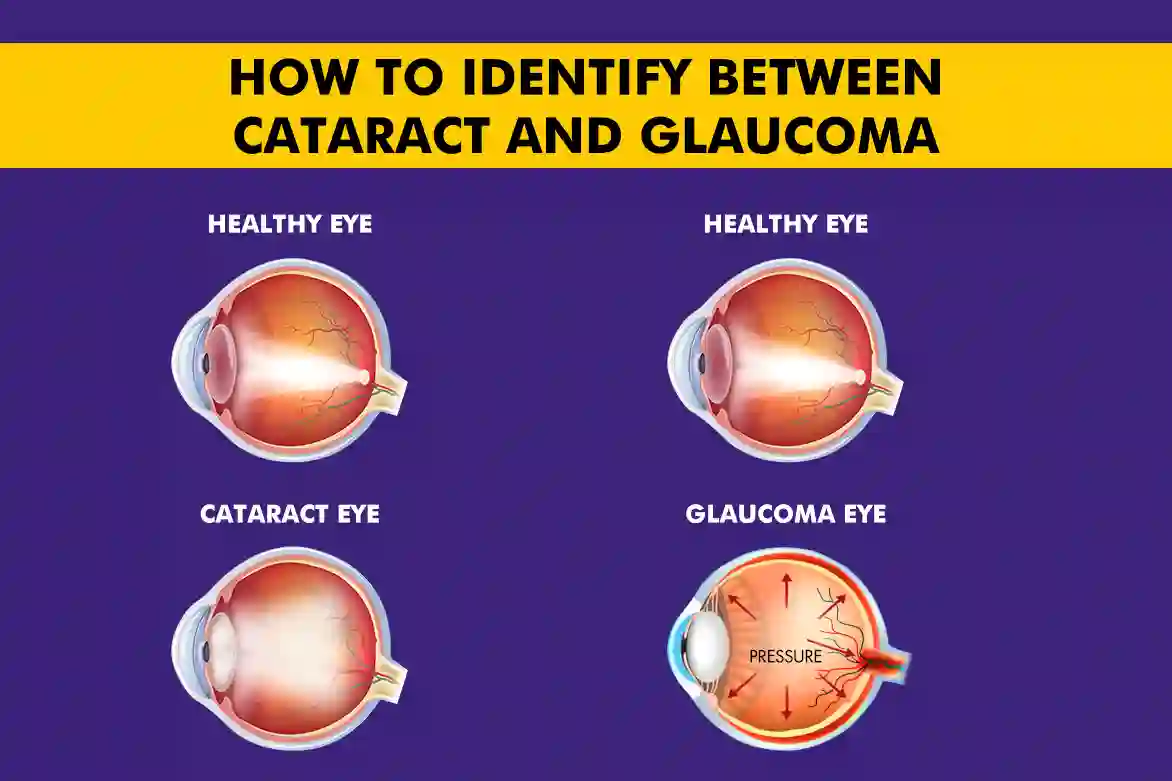
Glaucoma vs cataract can be confusing because cataract clouds the lens and is usually reversible with surgery, while glaucoma damages the optic nerve and needs lifelong pressure control.
People often mix them up since blur and glare can overlap, which can delay the right care. Knowing the difference between glaucoma and cataract helps you act in a timely manner.
In this blog, you’ll learn how they differ in symptoms, cause of vision loss, tests, and treatment, so that you can spot the right next step.
What Is a Cataract? (Definition, Symptoms, Causes)
A cataract is a clouding of the eye’s natural lens, the clear part that sits just behind the iris (the coloured part). When this lens turns cloudy, light can’t focus properly, so vision looks blurry, colours seem dull, and glare becomes bothersome.
Common symptoms of Cataract:
- Blurry or “foggy” vision that builds slowly
- Glare or halos around lights, worse at night
- Colours looking faded or yellowish
- Needing more light to read, frequent changes in the glasses power
Main causes and risks of Cataract:
- Ageing (the most common cause)
- Diabetes or long-term steroid use
- Smoking and long, unprotected sun exposure (UV light)
- Eye injury or prior eye surgery
- Family history (some people are more prone)
What Is Glaucoma? (Definition, Symptoms, Causes)
Glaucoma is a group of diseases that damage the optic nerve, the cable that carries images from your eye to your brain. This usually happens when intraocular pressure (IOP) is too high for that eye, but glaucoma can also occur with “normal” pressure. If left untreated, the damage builds gradually and can lead to permanent vision loss.
Common symptoms of Glaucoma:
- Gradual loss of side (peripheral) vision, like looking through a tunnel, over time
- Halos around lights, eye strain, or headaches
- Eye pain, redness, blurred vision, or sudden vision loss (an emergency in acute angle-closure)
Main causes and risks of Glaucoma:
- Higher-than-healthy eye pressure (IOP) or pressure spikes
- Ageing (risk rises after 40), family history of glaucoma
- Thin corneas, high myopia, or past eye injury
- Health conditions such as diabetes and hypertension
- Long-term steroid use (drops, tablets, or inhalers)
How Cataracts and Glaucoma Differ
Below are the key factors on how cataracts and glaucoma differ on the basis of cause of vision loss, symptoms, progression, treatment, outcome and management of the condition:
|
Condition |
Cause of vision loss |
Symptoms |
Progression |
Treatment |
Outcome |
Ongoing management |
|
Cataract |
Clouding of the eye’s natural lens (lens opacity) |
Blurry/foggy vision, glare/halos at night, faded colours, frequent power changes |
Slow, usually years; vision decline is reversible |
Cataract surgery (lens removal + IOL) |
Vision improves after surgery |
Routine checks post-op; no long-term meds needed for the cataract itself |
|
Glaucoma |
Damage to the optic nerve ( from high IOP) |
Early: silent; later: tunnel vision, halos, eye strain; acute angle-closure: pain/redness/halos/nausea |
Silent, gradual; vision loss is irreversible without timely control |
Pressure-lowering eye drops, laser, or surgery |
Goal is to preserve the remaining vision; lost vision cannot be restored |
Lifelong follow-up: IOP checks, visual fields, OCT; adherence to drops/plan is important |
How Doctors Diagnose Cataracts and Glaucoma
A good eye exam can tell these two apart. Your doctor first listens to your symptoms, then checks your vision and eye structures, and finally runs a few focused tests based on what they suspect.
Cataract: common tests
- Visual acuity: Checks how clearly you see at distance and near.
- Slit-lamp exam: Look at the front of the eye and the lens to see clouding.
- Dilated exam: Widens the pupil to inspect the lens and back of the eye more clearly.
- Additional tests (sometimes): Glare testing or photos to document how much light the lens scatters.
Glaucoma: common tests
- Tonometry (IOP): Measures intraocular pressure.
- Optic nerve exam / OCT RNFL: Doctor views the nerve; OCT scans the retinal nerve fiber layer (RNFL) for thinning.
- Visual field (perimetry): Maps side-vision loss of glaucoma.
- Gonioscopy: Checks the drainage angle where the iris meets the cornea (open vs closed).
- Pachymetry: Measures corneal thickness, which helps interpret pressure readings.
|
Simple rule of thumb Cataract testing focuses on the cloudy lens and how it blocks light, while glaucoma testing focuses on pressure, the drainage angle, the optic nerve, and side-vision. |
Treatment & Management: Condition-Specific Plans
Below are the treatment & management plans for Cataract and Glaucoma:
Cataract:
- When to treat: Plan surgery when blur, glare, or night driving limits daily life; earlier if the view to the retina is blocked or the other eye is weak.
- What surgery does: The cloudy lens is removed, and a clear intraocular lens (IOL) is placed. It’s an outpatient procedure; most people notice clearer vision within days.
- Lens choices: Standard monofocal is most common; toric can address astigmatism; premium options may reduce glasses for some tasks.
- Recovery & follow-up: Use prescribed drops, avoid eye rubbing/heavy lifting for a short time, and attend checks to confirm stable healing and vision.
Glaucoma:
- Treatment goal: Lower intraocular pressure (IOP) to a safe “target” level for that eye and keep it there.
- First-line: Eye drops (one or more classes) used daily and correctly; adherence matters.
- Laser options: SLT for open-angle glaucoma; laser iridotomy for narrow/angle-closure risk.
- Surgery when needed: Trabeculectomy, glaucoma drainage devices, or MIGS (minimally invasive glaucoma surgery) if drops/laser aren’t enough.
- Lifelong monitoring: Regular IOP checks, optic nerve/OCT scans, and visual fields to track change and adjust treatment early.
When to See a Doctor
Don’t wait if something feels wrong; some eye problems can’t be reversed once damage is done. See an eye doctor urgently if you notice:
- Sudden eye pain, redness, halos, or headache/nausea (possible acute angle-closure glaucoma).
- Rapid blur or a quick drop in vision in either eye.
- Family history of glaucoma or past high eye pressure.
- Age over 40 with risk factors like diabetes, high BP, steroid use, high myopia, or past eye injury.
- Glare at night or cloudy vision that interferes with daily tasks (possible cataract).
Conclusion
Both conditions can blur vision, but they are different: cataract clouds the lens and is usually reversible with surgery, while glaucoma damages the optic nerve and needs lifelong pressure control. Knowing the glaucoma vs cataract differences helps you match symptoms to the right tests and treatments.
Early checks matter because glaucoma loss is permanent, while cataract timing can be planned before it becomes disabling. With a clear diagnosis, most people can protect their sight well over the long term.
FAQs
How do I know if I have cataracts or glaucoma?
Cataracts primarily cause blurry or cloudy vision, while glaucoma leads to loss of peripheral vision. An eye exam can confirm the diagnosis.
Can cataracts and glaucoma occur together?
Yes, cataracts and glaucoma can occur together, and sometimes in the same eye. Therefore, doctors plan pressure control alongside timing for cataract surgery.
Is glaucoma more dangerous than cataracts?
Yes, glaucoma is more dangerous because vision loss from optic nerve damage is permanent, while cataract blur is usually reversible with surgery.
What tests differentiate cataracts from glaucoma?
The key tests are slit-lamp and dilated lens exam for cataracts, and IOP measurement, gonioscopy, OCT RNFL, and visual-field testing for glaucoma.
Are treatments for cataracts and glaucoma different?
Yes, cataracts are treated with lens-removal surgery (IOL implantation), while glaucoma is managed by lowering eye pressure with drops, laser treatment, or surgery over the long term.