|
Key Takeaways:
|
Major types of glaucoma are the different forms in which glaucoma harms the optic nerve, like primary glaucomas, open-angle glaucoma, normal-tension glaucoma, primary angle closure glaucoma, congenital glaucoma, secondary glaucoma, neovascular glaucoma, pigmentary glaucoma, exfoliation glaucoma, and uveitic glaucoma. The confusion is that early glaucoma is usually silent, so people feel normal, while slow, irreversible damage can still occur.
On this page, you’ll find information on the different types of glaucoma, key signs and tests, and first-line treatments for each type, so you know what to ask about at your next exam.
What is Glaucoma?
Glaucoma is an eye disease that damages the optic nerve, the cable that carries images from the eye to the brain. This damage relates to high eye pressure (IOP), but glaucoma can also happen when pressure is “normal” if the nerve is sensitive. The harm builds slowly and can cause permanent vision loss, so early checks and treatment make a big difference.
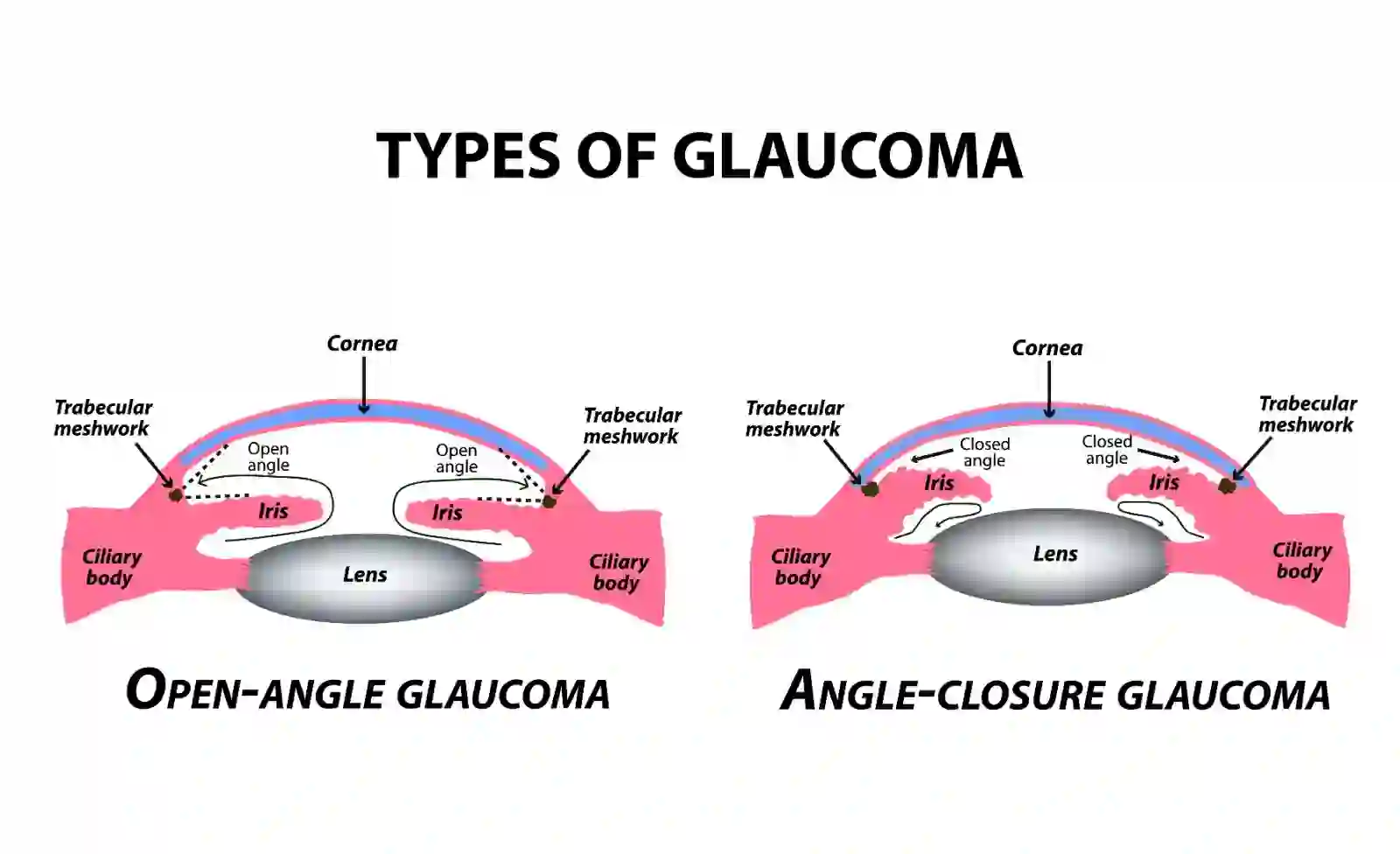
What Are the Types of Glaucoma?
Doctors group glaucoma into two types: Primary (no clear outside cause) and Secondary (caused by another eye/health problem). Below are the main types of Glaucoma:
|
Type |
Average age |
Key signs |
First-line treatment |
|
Primary Open-Angle Glaucoma (POAG) |
40+ |
Silent early loss of side vision |
Drops or SLT; add surgery if needed |
|
Normal-Tension Glaucoma (NTG) |
40+ |
Nerve damage despite “normal” IOP |
Lower target IOP with drops/SLT; close follow-up |
|
Primary Angle-Closure Glaucoma (PAC/PACG) |
40+ ( farsighted) |
Pain, redness, halos can be sudden |
Laser iridotomy ± meds; definitive angle treatment |
|
Primary Congenital/Pediatric Glaucoma |
Infants/children |
Large cloudy cornea, tearing, light sensitivity |
Surgery first; drops as support |
|
Neovascular Glaucoma |
Any (with diabetes/vein occlusion) |
Pain, redness, poor view; new vessels on the iris |
Treat cause + drops/laser; surgery needed |
|
Pigmentary Glaucoma |
Young–middle age ( myopic) |
Halos after exercise; pigment in angle |
Drops/SLT; activity/pose advice |
|
Exfoliation (Pseudoexfoliation) Glaucoma |
60+ |
Flaky deposits on lens/angle; higher IOP swings |
Drops/SLT; surgery if pressure labile |
|
Uveitic Glaucoma |
Any |
Inflammation, light sensitivity, and pressure swings |
Control inflammation + pressure; steroid caution |
|
Secondary (other causes) |
Any |
Depends on cause/trauma/meds |
Treat cause + pressure control |
Primary Glaucomas
Primary glaucomas are glaucoma types that don’t have an obvious external cause like trauma or another eye disease. The eye’s fluid outflow pathway or optic nerve tolerance is the main problem.
They usually start quietly and progress over time. Because early vision feels normal, regular exams are important to catch changes before damage builds up.
Symptoms:
- No symptoms at first; later, tunnel vision or patchy side-vision loss
- Occasional halos or eye strain, especially in dim light
- In angle-closure forms: pain, redness, halos, headache/nausea (urgent)
Treatment options:
- Pressure-lowering drops are the first line in many cases
- Laser (SLT for open angles; iridotomy for narrow angles)
- Surgery if drops/laser are not enough (MIGS, trabeculectomy, drainage devices)
Primary Open-Angle Glaucoma (POAG)
Primary Open-Angle Glaucoma, or POAG, is the most common type of glaucoma. The drainage angle is open, but fluid doesn’t leave efficiently, so pressure harms the optic nerve over time. Damage is slow and painless, so people notice vision loss late. Early detection and a clear target IOP help protect sight.
Symptoms
- Silent early loss of side vision
- Glare/halos or eye fatigue later on
- Central vision affected only in the advanced stages
Treatment options .
- Drops (prostaglandin analogues first; add others as needed)
- SLT laser to improve outflow (first-line or add-on)
- Surgery (MIGS/trabeculectomy/drainage device) if control is inadequate
Normal-Tension Glaucoma (NTG)
Normal Tension Glaucoma or NTG is glaucoma where optic nerve damage occurs despite “normal” clinic IOP. Some nerves are more pressure-sensitive, and blood-flow factors may contribute. Care focuses on lowering IOP below normal for that person and watching the nerve and visual fields closely.
Symptoms.
- Similar to POAG: gradual side-vision loss
- No pain or redness
- May be linked with cold hands/migraines/sleep apnea (vascular clues)
Treatment options
- Lower target IOP with drops and/or SLT
- Address vascular risks (sleep apnea, BP extremes) where relevant
- Surgery if progression continues at low pressures
Primary Angle-Closure Glaucoma (PAC/PACG)
Primary Angle-Closure Glaucoma, also known as PAC or PACG, occurs when the iris blocks the drainage angle, preventing fluid from exiting and allowing pressure to rise quickly. This can be an emergency when it is sudden. Some people have narrow angles that close slowly over time; others have an acute attack with pain and halos.
Symptoms
- Severe eye pain, redness, blurred vision, halos
- Headache, nausea/vomiting in acute attacks
- In chronic narrow angles: intermittent blur or halos in dim light
Treatment options
- Laser iridotomy to open a new fluid pathway
- Pressure-lowering drops and short-term meds during attacks
- Definitive angle procedures or cataract surgery if needed
Congenital (Pediatric) Glaucoma
Congenital (Pediatric) Glaucoma forms appear in infants or children due to abnormal development of the drainage system. Pressure damages the young eye quickly. Early recognition and prompt surgery are key to protecting vision and development.
Symptoms
- Large, cloudy cornea, tearing, light sensitivity
- Frequent eye rubbing, irritability
- One eye may look bigger than the other
Treatment options
- Surgery first (goniotomy/trabeculotomy; other procedures as needed)
- Supportive drops as advised
- Close follow-up for vision development (glasses/patching when needed)
Secondary Glaucoma
Secondary glaucomas happen because of another problem, such as inflammation, trauma, blocked veins, new vessels, lens issues, or steroid medicines. Treatment always targets both the pressure and the underlying cause.
Symptoms
- It vary by cause: pain/redness or gradual blur
- Pressure that is hard to control or fluctuates
- Signs of the underlying issue (e.g., pigment, flakes, inflammation)
Treatment options
- Treat the cause (e.g., control diabetes/uveitis; stop/adjust steroids)
- Pressure-lowering drops/laser
- Surgery if pressure stays high
Neovascular Glaucoma
Neovascular Glaucoma happens when fragile blood vessels grow on the iris and drainage angle, blocking outflow. It follows severe diabetic eye disease or retinal vein occlusion. This type is aggressive and needs combined retina and glaucoma care.
Symptoms
- Pain, redness, and reduced vision
- Poor view of the angle with abnormal surface vessels
- High, resistant IOP
Treatment options
- Treat the retina (anti-VEGF injections, laser) + pressure control
- Multiple drops and sometimes cyclodestructive laser
- Surgery (tube shunt/trabeculectomy) frequently required
Pigmentary Glaucoma
Pigmentary glaucoma occurs when pigment from the iris rubs off and clogs the drainage meshwork, thereby increasing pressure. It’s more common in young to middle-aged people with myopia. Activity and posture can affect symptoms; management aims to control pressure and reduce pigment dispersion.
Symptoms
- Halos or blur after exercise
- Pigment seen in the angle/cornea on exam
- Gradual side-vision loss if untreated
Treatment options
- Pressure-lowering drops; consider SLT
- Lifestyle advice (avoid frequent deep head-down or high-impact jarring if it provokes spikes)
- Surgery if control is inadequate
Exfoliation (Pseudoexfoliation) Glaucoma
Exfoliation (Pseudoexfoliation) Glaucoma occurs when flaky, dandruff-like material accumulates on the lens and angle, making pressure control more challenging. It’s more common with age and may progress faster than POAG. IOP can swing widely, so close monitoring is important.
Symptoms
- Variable or high IOP with “flakes” seen on exam
- Increasing need for medicines over time
- Gradual side-vision loss if untreated
Treatment options
- Drops (more than one class)
- SLT can help, but may wane; repeat or combine treatments
- Surgery sooner if swings are large or nerve shows change
Uveitic Glaucoma
Uveitic Glaucoma happens when inflammation inside the eye (uveitis) blocks or scars the outflow pathway and stiffens the drainage meshwork. Steroid treatment, while useful for inflammation, can also raise IOP. Management balances controlling inflammation and lowering pressure.
Symptoms
- Light sensitivity, redness, discomfort
- Pressure that rises during flares or steroid use
- Blurred vision that waxes and wanes
Treatment options
- Control uveitis (steroid-sparing strategies when possible)
- Pressure-lowering drops/laser; steroid caution and monitoring
- Surgery if scarring or high IOP persists
Conclusion
Glaucoma isn’t one disease; its types of glaucoma differ by how the drainage angle and optic nerve are affected. Some forms stay silent for years, while others, like angle-closure or neovascular glaucoma, can worsen quickly. Treatment aims to lower pressure and protect the nerve, using drops, laser therapy, or surgery, depending on the type.
With regular checks and timely care, most people can slow or stop further damage.
FAQs
What are the different types of glaucoma?
The different types of glaucoma are primary open-angle, normal-tension, primary angle-closure, congenital/pediatric, and secondary forms, including neovascular, pigmentary, exfoliation (pseudoexfoliation), and uveitic.
What are the different classifications of glaucoma?
The main classification of glaucoma is primary, which has no clear external cause; open-angle or angle-closure and secondary due to other problems like steroids, inflammation, new vessels, trauma, or lens issues.
What is Grade 4 glaucoma?
Grade 4 glaucoma means an end-stage/advanced glaucoma in staging systems with severe visual-field loss; naming varies by clinic, so your report’s scale should be read in context.
Which type of glaucoma is more serious?
Angle-closure (especially acute) and neovascular glaucoma are more urgent and vision-threatening, but any glaucoma is serious if pressure isn’t controlled.
Is glaucoma 100% curable?
No, glaucoma isn’t 100% curable; treatment lowers eye pressure to protect the optic nerve, but vision already lost cannot be restored.
What is high-risk glaucoma?
High-risk glaucoma means a greater chance of damage due to factors like very high IOP, thin corneas, strong family history, certain ethnicities, diabetes, high myopia, or steroid response.
What is the difference between primary glaucoma and secondary glaucoma?
Primary glaucoma develops without an external cause (open-angle or angle-closure). In contrast, secondary glaucoma occurs due to another condition, such as inflammation, steroid use, pigment or exfoliation material, trauma, or the formation of new blood vessels.